

CAUSES
- Shape of acromion bone
- Bone spur
- Muscle imbalance
NONOPERATIVE TREATMENT
- Physical therapy
- Injection (PRP or cortisone)
- Rest
- Physical therapy
PREOP
- X-ray
- MRI Scan--Evaluate Rotator Cuff
- Trial of nonoperative treament
RECOVERY
- 10 days suture removal
- 3-5 days sling
- 3 months physical therapy 2 x per week.
- Expectation is excellent range of motion and minimal to no pain with return to full activity
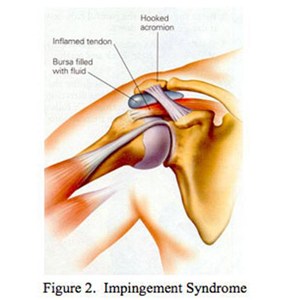
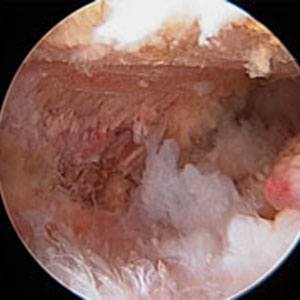
TECHNIQUE
The treatment of impingement syndrome surgically is to shave the undersurface of the acromion bone to create a smooth gliding surface and to remove bursitis and inflammation.
DAY OF SURGERY
- Nerve block anesthesia
- 1 hour surgery
- Outpatient
WHEN TO HAVE SURGERY?
- Significant pain
- Loss of motion
- Poor shoulder function
- Failed conservative treatment (PT and injection)
- Night pain
Questions?
Email Dr. Gamradt - [javascript protected email address]
[javascript protected email address] Office Phone:



