

Overview
The rotator cuff is a series of 4 muscles in the shoulder that form a cuff of tissue around the humerus bone in the shoulder joint. These muscles provide rotational strength to the shoulder. Tears in the tendons of these muscles are called rotator cuff tears. The most commonly affected muscle is the supraspinatus.
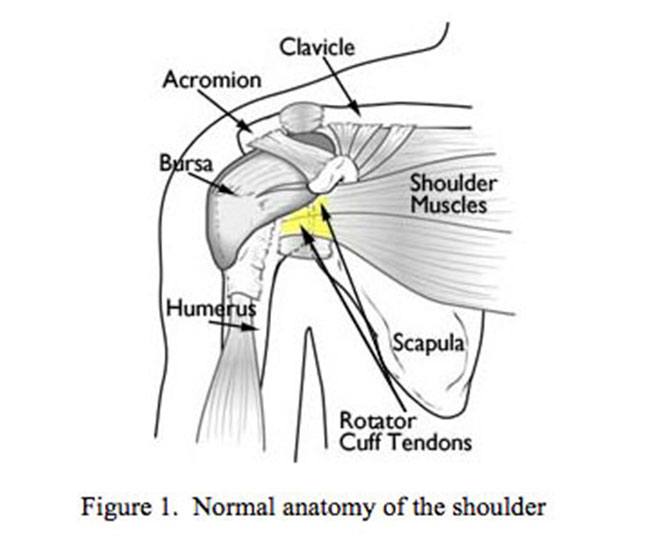
Figure 1. Normal anatomy of the shoulder
There are two causes of rotator cuff tearse
- Extrinsic compression – A combination of susceptible anatomy and a lifetime of wear and tear can cause mechanical abrasion and impingement of the supraspinatus on the acromion bone.
- Intrinsic degeneration – Aging of the rotator cuff tendon. As we age, the quality of our tendons and the blood supply to the tendons diminishes, making the tendons susceptible to tearing.
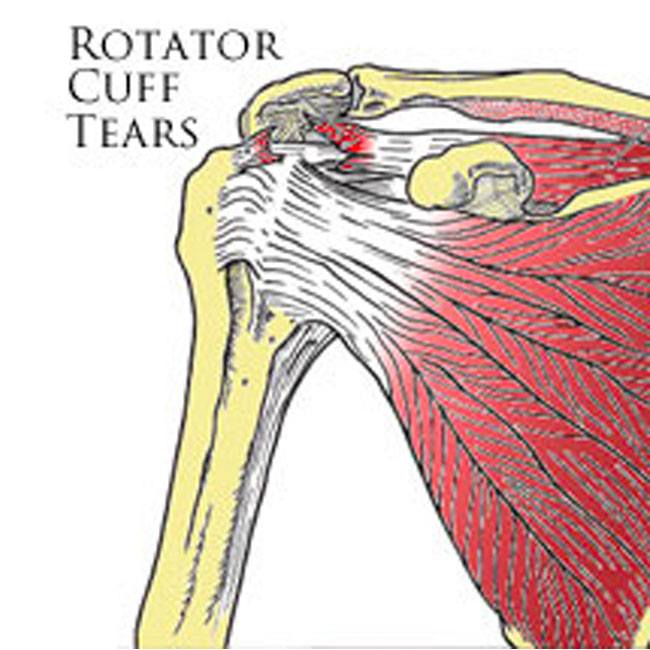
Figure 2. Rotator Cuff Tear
Symptoms
The symptoms of rotator cuff tears are as follows
- Pain: Rotator cuff tears cause an aching pain in both the front of the shoulder and also the outer side of the upper arm. The pain is often dull at rest, exacerbated by overhead activity, and severe at night
- Weakness: Due to detachment of the muscle from bone, the shoulder will be weak, especially while lifting and with overhead activity.
- Lack of Mobility: Some movements may pinch the tendon in such a way that the shoulder will not be able to rotate sufficiently to allow the arm to complete the action. Other motions may simply be too painful.
Evaluation
- Physical exam: Is very sensitive at picking up weakness associated with rotator cuff tears.
- X-ray: Obtained to screen for arthritis and bone spurs
- MRI: Gold standard for characterizing size, location, and reparability of rotator cuff tear.
- Ultrasound: used when MRI cannot be obtained (claustrophobia, pacemaker).
Initial Treatment
Initial treatment for rotator cuff tears is usually nonoperative and should include the following conservative treatment measures
- Rest: Because the shoulder is not a weight bearing joint like the knee, simply modifying one’s activities can improve symptoms
- Medications: Tylenol or anti-inflammatories can help with symptoms
- Injections: Steroid injections can provide temporary relief.
- Physical therapy: Range of motion exercises and strengthening can improve symptoms.
- Surgery: Rotator cuff tears do not heal on their own. However, there is a chance that with physical therapy and the modalities listed above, that symptoms from small tears can improve to the point where the patient chooses to not have surgery. Symptomatic small and medium sized tears, most large tears, and acute tears that occur due to trauma are commonly treated with surgery. The decision to have surgery for a rotator cuff tear is a commitment to a long rehabilitation process. In certain cases, due to muscle atrophy and tendon retraction, the tear is obviously not repairable based on MRI criteria. This condition is called ‘irreparable rotator cuff tear’ and precludes an anatomic repair. The mainstays of treatment for irreparable rotator cuff tears are physical therapy and injections, but certain patients are candidates for arthroscopic debridement, augmentation with a graft, tendon transfers, or reverse shoulder replacement.

Figure 3A and 3B: Metal and Biocompatible suture anchors used in rotator cuff repair. These devices are inserted into bone to act as a fixation point for the rotator cuff to be reattached to bone. Figure 3c: shows a large crescent shaped rotator cuff tear. Figure 3d: The rotator cuff is repaired to bone arthroscopically to bone with a double row configuration.

Figure 3B: Sometimes, if tissue quality and tear configuration allow, a double row of suture anchors is used to add strength to the repair. Below are some images that illustrate rotator cuff repair.
Surgical Treatment
Arthroscopic Rotator Cuff Repair
Surgical treatment is very effective at repairing the rotator cuff and eliminating the underlying cause (impingement syndrome). Pain relief is excellent and strength is usually gained. Dr. Gamradt performs repairs rotator cuff tears arthroscopically through a minimally invasive approach.
Surgery is performed arthroscopically in the outpatient setting (same day surgery). General or nerve block anesthesia is administered. Three to four small incisions (5 mm) are made in the shoulder to allow a camera and specialized instruments into the shoulder. Inflamed bursa and bone spurs are removed arthroscopically, creating space for the rotator cuff muscles and eliminating impingement. Suture anchors are utilized for the repair. Suture anchors are small metal or bioabsorbable screws that have two sutures each attached to them. After mobilizing the tendon so that it can be anatomically repaired, suture anchors are inserted in bone. The sutures from the anchors are passed through the tendon and used to repair the rotator cuff securely to the bone arthroscopically. Sometimes, if tissue quality and tear configuration allows, a double row of suture anchors is used to add strength to the repair. Below are some images that illustrate rotator cuff repair.
Figure 3A and 3B: Metal and Biocompatible suture anchors used in rotator cuff repair. These devices are inserted into bone to act as a fixation point for the rotator cuff to be reattached to bone. Figure 3C: shows a large crescent shaped rotator cuff tear. Figure 3D: The rotator cuff is repaired to bone arthroscopically to bone with a double row configuration.
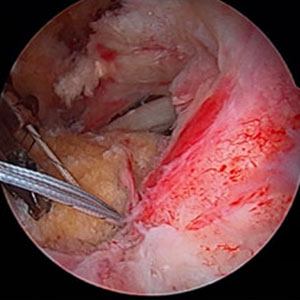
Figure 3C
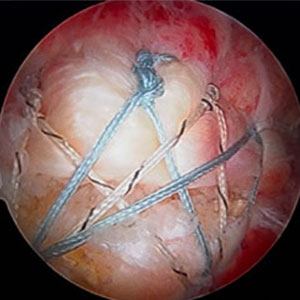
Figure 3D

Figure 4A: Large anterior acromial bone spur associated with rotator cuff tear
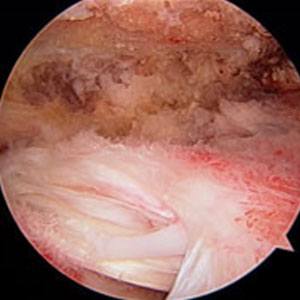
Figure 4B: After removal of spur
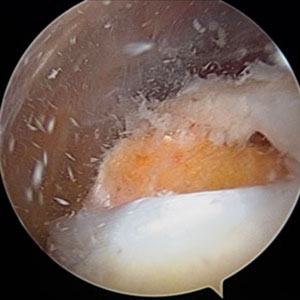
Figure 4C: Crescent shaped rotator cuff tear

Figure 4D: Insertion handle of biocompatible suture anchor

Figure 4E: After passage of sutures from suture anchor through rotator cuff

Figure 4F: After passage of sutures from suture anchor through rotator cuff, lateral view
What to Expect
Pre-op
- An MRI and x-rays of your shoulder will be ordered to evaluate for bone spurs, arthritis, and for the location, size, and reparability of the rotator cuff.
- If you have any medical problems, you will need a consultation with your PMD and/or cardiologist prior to surgery to ensure that you are safe for anesthesia.
Day of Surgery/Hospital Stay
- Nothing to eat or drink past midnight the night before surgery
- Surgery lasts 2-3 hours depending on complexity and is performed in the outpatient setting.
- Surgery is performed under general anesthesia or nerve block anesthesia (regional)
- Your arm will be in a sling postoperatively for 6 weeks.
- You will start exercises the day following surgery to move the shoulder passively.

Figure 4G Completed double row repair
Post-Op/Rehab
- Post-op visits:
- 2 weeks: suture removal, check motion and ensure proper performance of Seth C. Gamradt, MD, Orthopedic Surgeon, Beverly Hills, Los Angeles, CA exercises, start physical therapy
- 6 weeks: Discontinue Sling. Advanced physical therapy
- 12 weeks: Check range of motion and strength
- 16-20 weeks: Stop formal physical therapy and begin Seth C. Gamradt, MD, Orthopedic Surgeon, Beverly Hills, Los Angeles, CA program
- 24 weeks: final checkup.
- Physical therapy usually lasts 16 weeks and is divided into three phases
- 0-6 weeks: sling and passive motion
- 6-12 weeks: active motion
- 12-16 weeks: strengthening
- Even though most patients complete formal physical therapy 4-5 months post-surgery. Final healing is probably not complete until one year after surgery.



