

Overview
An acromioclavicular (AC) joint separation is also referred to as a shoulder separation. An AC separation is a very common injury in sports and in falls onto the shoulder from a bike for example. The AC joint is the connection between the scapula (shoulder blade) and the clavicle (collarbone). An AC separation is not a shoulder dislocation. During the injury, the clavicle is forced upward and can be elevated in relation to the acromion. Falls directly on the shoulder are the usual cause of this injury. Football, biking, skiing, snowboarding and other sports which allow contact with the shoulder and the ground are the commonest causes of this injury.
During the injury varying degrees of injury to the structures that hold the AC joint together occur. The AC joint capsule and two ligaments, the coracoclavicular ligaments, hold the clavicle down level with the acromion.
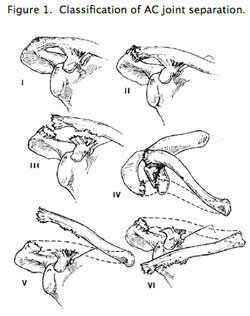
AC joint separations are graded from mild to severe, depending on which ligaments are sprained or torn and how high the clavicle is elevated in relation to the acromion. The mildest type of injury is a simple sprain of the AC joint capsule (grade I). A grade 2 separation is a partial tear of the coracoclavicular ligaments with partial elevation of the clavicle. A complete tear of the AC ligaments and the coracoclavicular ligaments is a results in 100 % elevation of the clavicle with respect to the acromion. Grade 4, 5, and 6 separations are severe injuries with high degree of displacement of the clavicle with respect to the acromion and usually require surgery. Figure one summarizes the classification of AC joint injuries.
Treatment
Treatment of AC joint separations depends on the type (severity) of the AC joint injury. This classification is based on the severity of the injury (degree of elevation of the clavicle with respect to the acromion on x-ray and clinical exam.
- Type 1 and 2 AC separations: These injuries are mild and are universally treated without surgery. Elevation of the clavicle is mild with only a small prominence on top off the shoulder. Rest, ice, anti-inflammatory medication, and occasionally a cortisone injection are used to treat the initial pain and swelling and return to sport us usually between 1-8 weeks depending on the severity of the trauma and the energy of the injury. Late sequelae such as arthritis of the AC joint can occur, but this is rare and can require many years to develop.
- Type 3 AC separations: These injuries are usually higher energy and result in significant displacement of the clavicle (100%) with respect to the acromion. The elevated clavicle results in a prominence on top of the shoulder which is initially painful. Treatment of type 3 AC separations is more controversial. Initial treatment is similar to type 1 and 2 injuries with rest, ice, anti-inflammatory medication, and occasionally a cortisone injection. If the joint is still painful with abnormal mobility and clicking after nonoperative treatment, surgery is commonly recommended to reconstruct the joint and restore and improve the relationship between the acromion and clavicle. If the pain in the joint goes away and shoulder function is good, most patients and physicians choose to accept the bump (prominence) on the shoulder rather than opt for surgery. Most patients who elect to have surgery continue to have a painful popping sensation in the shoulder with activity that persists despite rest and rehabilitation. A standard period of waiting prior to deciding on whether or not to operate on a type 3 AC separation is about 3 months. However, some patients choose to have surgery on the shoulder immediately if they know they will be bothered by the dislocated clavicle in the future.
- Type 4, 5, and 6 AC separations: These injuries result in severe displacement of the clavicle with respect to the acromion and surgery is usually recommended immediately within the first three weeks after injury.
Surgery
The type of surgery performed to reconstruct the AC joint after a severe separation (Type 3-6) is controversial. Recently, there has been a renewed focus on improving the surgery to reconstruct the AC joint. This is called an anatomic AC joint reconstruction and was well studied both clinically and in the laboratory by a physician named Dr. Mazzocca at the University of Connecticut. Severe injury to the AC joint results in a tear of not only the AC joint capsule but also the coracoclavicular ligaments which serve as a strong connection from the coracoid process to the clavicle.
During this surgery, the torn coracoclavicular ligaments are reconstructed (replaced) using cadaver tissue. The cadaver graft is placed in the exact location of the torn ligaments and is fixed with bio-compatible screws. The new ligaments heal and serve to restore the normal anatomy of the shoulder. Dr. Gamradt performs part of this operation arthroscopically, but the graft must be secured through a small open incision.
Rehabilitation after the surgery involves six weeks in a sling followed by three months of supervised physical therapy to restore motion and strength. Return to contact sports is probably not advisable until 5-6 months after surgery. Despite surgery, the clavicle can still remain prominent and the surgery is not 100 percent successful. Recurrence of the AC separation can also occur, especially in contact athletes.
Arthroscopic Assisted Anatomic AC Joint Reconstruction Pictures
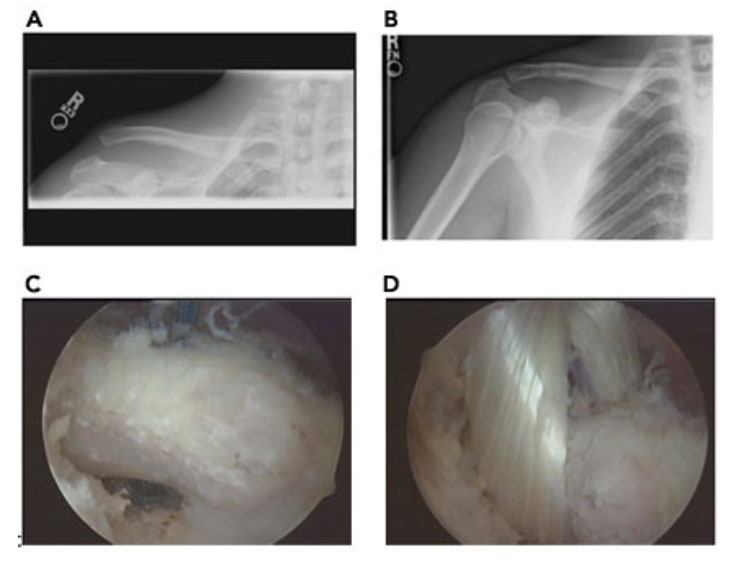
Figure 2A. Type 5 AC separation with 200% elevation of clavicle with respect to AC joint
Figure 2B. Postoperative x-ray after anatomic coraco-clavicular ligament reconstruction with tibialis anterior allograft.
Figure 2C: Arthroscopic exposure of coracoid process
Figure 2D: Arthroscopic passage of coracoclavicular ligament graft around coracoid process to restore normal AC joint anatomy



